Table Of Content
These preexisting differences between the groups—and not the financial education program—could explain the observed differences in outcomes. Therefore, the study is not eligible for a moderate causal evidence rating, the highest rating available for nonexperimental designs. For example, a manufacturing company might measure its workers’ productivity each week for a year. In an interrupted time series-design, a time series like this one is “interrupted” by a treatment. In one classic example, the treatment was the reduction of the work shifts in a factory from 10 hours to 8 hours (Cook & Campbell, 1979)[5].
Workplace financial education and change in financial knowledge: A quasi-experimental approach (Horwitz et al.,
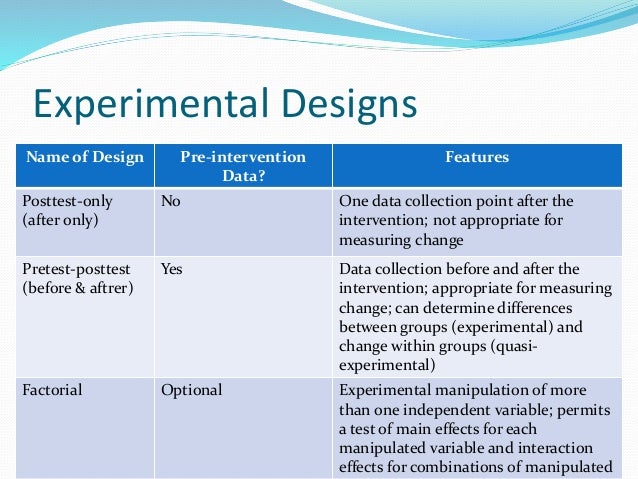
This design involves collecting data on the dependent variable(s) over a period of time, both before and after an intervention or event. The researcher can then determine whether there was a significant change in the dependent variable(s) following the intervention or event. The first common difference that sets apart implementation RCTs from more traditional clinical trials is the primary research question they aim to address. For most implementation trials, the primary research question is not the extent to which a particular treatment or evidence-based practice is more effective than a comparison condition, but instead the extent to which a given implementation strategy is more effective than a comparison condition.
The differential influence of self-construal on the effect of self-efficacy on the help-seeking process: A quasi ... - ScienceDirect.com
The differential influence of self-construal on the effect of self-efficacy on the help-seeking process: A quasi ....
Posted: Fri, 12 Jan 2024 15:31:03 GMT [source]
Researchers
The first documented clinical trial was conducted in 1747 by James Lind, a royal navy physician, who tested the hypothesis that citrus fruit could cure scurvy. Since then, based on foundational work by Fisher and others (1935), the randomized controlled trial (RCT) has emerged as the gold standard for testing the efficacy of treatment versus a control condition for individual patients. Randomization of patients is seen as a crucial to reducing the impact of measured or unmeasured confounding variables, in turn allowing researchers to draw conclusions regarding causality in clinical trials. Again, if students in the treatment condition become more negative toward drugs, this could be an effect of the treatment, but it could also be a matter of history or maturation. In a pretest-posttest design, the dependent variable is measured once before the treatment is implemented and once after it is implemented. Stepped wedge designs (SWDs) involve a sequential roll-out of an intervention to participants (individuals or clusters) over several distinct time periods (5, 7, 22, 24, 29, 30, 38).
Example 2: Determining the effectiveness of teaching modern leadership techniques in start-up businesses
In addition, ITS designs can increase power by making full use of longitudinal data instead of collapsing all data to single pre- and post-intervention time points. The use of longitudinal data can also be helpful for assessing whether intervention effects are short-lived or sustained over time. The authors did not account for other factors that could have affected the difference between the treatment and comparison groups, such as race/ethnicity. Also, the groups were significantly different in age, but the authors did not control for the differences in the analyses.
Causal Evidence Rating
Adaptive designs could potentially be incorporated into both SMART designs and stepped wedge studies, as well as traditional RCTs to further advance implementation science (Cheung et al., 2015). Ideally, these and other innovations will provide researchers with increasingly robust and useful methodologies for answering timely implementation science questions. While two-arm RCTs can be used to evaluate comparative effectiveness, trials focused on optimizing implementation support may use alternative experimental designs (Collins et al., 2005; Collins et al., 2007). For example, in certain clinical contexts, multi-component “bundles” of implementation strategies may be warranted (e.g. a bundle consisting of clinician training, technical assistance, and audit/feedback to encourage clinicians to use a new evidence-based practice).
Features of the Study
But if the intervention under study incorporates an accepted, well-established therapeutic intervention, or if the intervention has either questionable efficacy or safety based on previously conducted studies, then the ethical issues of randomizing patients are sometimes raised. In the area of medical informatics, it is often believed prior to an implementation that an informatics intervention will likely be beneficial and thus medical informaticians and hospital administrators are often reluctant to randomize medical informatics interventions. In addition, there is often pressure to implement the intervention quickly because of its believed efficacy, thus not allowing researchers sufficient time to plan a randomized trial. Third, given their focus, implementation RCTs are frequently cluster-randomized (i.e. with sites or clinics as the unit of randomization, and patients nested within those sites or clinics).
Perhaps an antidrug program aired on television and many of the students watched it, or perhaps a celebrity died of a drug overdose and many of the students heard about it. Participants might have changed between the pretest and the posttest in ways that they were going to anyway because they are growing and learning. If it were a yearlong program, participants might become less impulsive or better reasoners and this might be responsible for the change.
Quasi-experimental Designs That Use a Control Group but No Pretest
The authors administered a 50-question survey to participants and non-participants within 72 hours of the program start (pre-survey) and end (post-survey). The survey questions assessed financial knowledge, financial satisfaction, money beliefs, and money behaviors. The authors conducted statistical analyses to compare differences in outcomes between program participants and non-participants.
Shadish et al.4 discuss 17 possible designs, with seven designs falling into category A, three designs in category B, and six designs in category C, and one major design in category D. Thus, for simplicity, we have summarized the 11 study designs most relevant to medical informatics research in ▶. Using the pharmacy order-entry system example, it may be difficult to randomize use of the system to only certain locations in a hospital or portions of certain locations. For example, if the pharmacy order-entry system involves an educational component, then people may apply the knowledge learned to nonintervention wards, thereby potentially masking the true effect of the intervention.
The advantage of this design over design C2 is that it demonstrates reproducibility in two different settings. This study design is not limited to two groups; in fact, the study results have greater validity if the intervention effect is replicated in different groups at multiple times. In the example of a pharmacy order-entry system, one could implement or intervene in the MICU and then at a later time, intervene in the SICU. This latter design is often very applicable to medical informatics where new technology and new software is often introduced or made available gradually.
Data is collected on all clusters such that they each contribute data during both control and intervention time periods. The order in which clusters receive the intervention can be assigned randomly or using some other approach when randomization is not possible. For example, in settings with geographically remote or difficult-to-access populations, a non-random order can maximize efficiency with respect to logistical considerations. Quasi-experimental research designs are the most widely used research approach employed to evaluate the outcomes of social work programs and policies. This new volume describes the logic, design, and conduct of the range of such designs, encompassing pre-experiments, quasi-experiments making use of a control or comparison group, and time-series designs.
Professional values at the beginning of medical school: a quasi-experimental study - BMC Medical Education - BMC Medical Education
Professional values at the beginning of medical school: a quasi-experimental study - BMC Medical Education.
Posted: Fri, 08 Mar 2024 08:00:00 GMT [source]
Specifically, we describe four quasi-experimental designs – one-group pretest–posttest designs, non-equivalent group designs, regression discontinuity designs, and interrupted time-series designs – and their statistical analyses in detail. Both simple quasi-experimental designs and embellishments of these simple designs are presented. Potential threats to internal validity are illustrated along with means of addressing their potentially biasing effects so that these effects can be minimized.
This method is used to compare the outcomes of participants who fall on either side of a predetermined cutoff point. This method can help researchers determine whether an intervention had a significant impact on the target population. This design involves measuring the dependent variable(s) before and after an intervention or event, but without a control group.
The pretest-posttest design is much like a within-subjects experiment in which each participant is tested first under the control condition and then under the treatment condition. It is unlike a within-subjects experiment, however, in that the order of conditions is not counterbalanced because it typically is not possible for a participant to be tested in the treatment condition first and then in an “untreated” control condition. Ethical considerations typically will not allow random withholding of an intervention with known efficacy. Thus, if the efficacy of an intervention has not been established, a randomized controlled trial is the design of choice to determine efficacy.
For example, typical implementation outcomes might include the number of patients who receive the intervention, or the number of providers who administer the intervention as intended. A variety of evaluation-oriented implementation frameworks may guide the choices of such measures (e.g. RE-AIM; Gaglio et al., 2013; Glasgow et al., 1999). Hybrid implementation-effectiveness studies attend to both effectiveness and implementation outcomes (Curran et al., 2012); these designs are also covered in more detail elsewhere in this issue (Landes, this issue). While the basic ITS design has important strengths, the key threat to internal validity is the possibility that factors other than the intervention are affecting the observed changes in outcome level or trend. Changes over time in factors such as the quality of care, data collection and recording, and population characteristics may not be fully accounted for by the pre-intervention trend.








No comments:
Post a Comment